Cobb Angle in Scoliosis: What It Means, How It Is Measured, and Why It Matters
Understanding the Cobb Angle
If you or your child has recently been diagnosed with scoliosis, one of the first terms you will likely hear is the Cobb angle.
The Cobb angle is the internationally accepted gold standard used by healthcare professionals to measure and quantify the severity of a spinal curvature. It is the primary measurement used to diagnose scoliosis, monitor progression, and guide treatment decisions.
In simple terms, the Cobb angle tells us how much the spine curves when viewed from the front or back on an X-ray.
A spinal curve must measure 10 degrees or greater before a formal diagnosis of scoliosis can be made.
However, while the Cobb angle is extremely important, it does not tell the entire story. Particularly in adults, factors such as pain, posture, balance, spinal degeneration, and quality of life may be even more important than the number itself.
What Is the Cobb Angle?
The Cobb angle is a measurement expressed in degrees that quantifies the amount of side-to-side spinal curvature.
It was first described by orthopedic surgeon Dr. John Cobb in 1948 and remains the standard measurement used worldwide today.
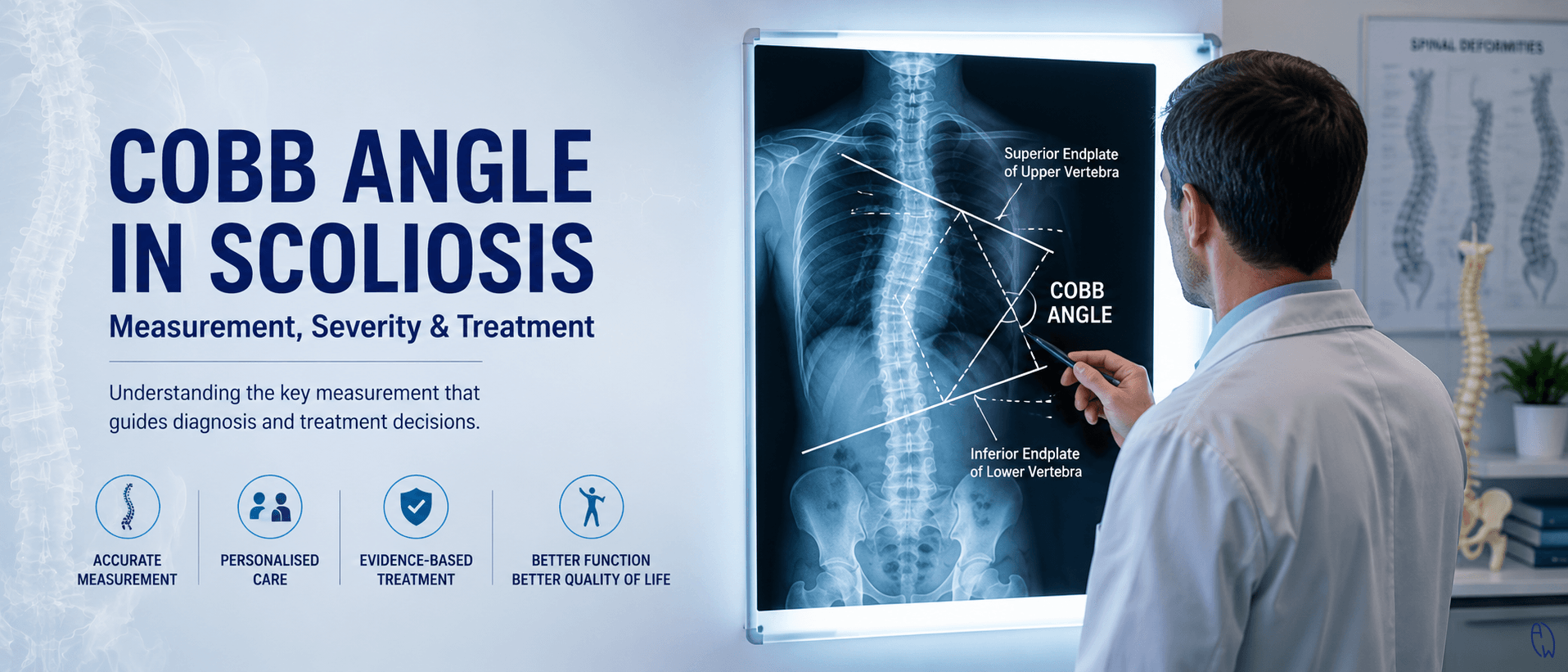
When reviewing a standing spinal X-ray, the clinician identifies:
-
The most tilted vertebra at the top of the curve
-
The most tilted vertebra at the bottom of the curve
Lines are drawn along the endplates of these vertebrae. The angle formed where these lines intersect (or where perpendicular lines intersect) is known as the Cobb angle.
Why Is 10 Degrees Important?
A spinal asymmetry below 10 degrees is generally not considered scoliosis.
Once the curve reaches 10 degrees or greater, scoliosis can be formally diagnosed.
This threshold is recognised internationally and is used in clinical practice and research studies around the world.
How Scoliosis Is Classified by Cobb Angle
The severity of scoliosis is commonly classified according to the measured Cobb angle.
Mild Scoliosis
10°–24°
Mild scoliosis often shows minimal physical changes and may not cause symptoms.
Many individuals with mild scoliosis simply require observation and periodic monitoring to ensure the curve does not worsen.
Learn more about early detection in our article on adolescent scoliosis and growth spurts. https://allwellscoliosis.com/articles/growth-spurts-curve-changes-and-what-every-parent-must-monitor
Moderate Scoliosis
25°–39°
At this stage, the risk of progression becomes more significant, especially in growing children and adolescents.
Physical changes such as uneven shoulders, rib prominence, or waist asymmetry often become more noticeable.
For children who are still growing, scoliosis-specific bracing may be recommended to reduce the risk of progression.
Severe Scoliosis
40°–50° and above
Severe scoliosis can have a greater impact on posture, spinal mechanics, and overall quality of life.
Curves in this range may continue to progress over time, even after skeletal maturity.
In some cases, spinal surgery may be considered, particularly if the curve continues worsening or causes significant symptoms.
How the Cobb Angle Influences Treatment Decisions
One of the most important roles of the Cobb angle is helping clinicians determine the most appropriate treatment pathway.
However, the treatment recommendation depends not only on the degree of curvature but also on factors such as age, growth potential, symptoms, and overall spinal function.
Observation
Curves less than 25 degrees are typically monitored regularly.
This may involve:
-
Periodic clinical assessments
-
Repeat X-rays when necessary
-
Monitoring growth spurts in children and adolescents
Observation allows clinicians to identify progression early before more aggressive interventions become necessary.
Bracing
For growing children and adolescents, curves between approximately 20 and 40 degrees may benefit from scoliosis-specific bracing.
The primary goal of bracing is not to permanently straighten the spine but to prevent the curve from worsening during growth.
Research consistently shows that appropriately designed braces can significantly reduce progression risk.
Read more in our comprehensive guide to scoliosis bracing https://scolicare.com/scolibrace
Scoliosis-Specific Exercise
Exercise plays an increasingly important role in scoliosis management.
Unlike general fitness programs, scoliosis-specific exercises are designed to:
-
Improve postural awareness
-
Address asymmetrical muscle activation
-
Improve spinal stability
-
Support brace effectiveness
-
Improve movement patterns and function
Many patients benefit from combining exercise therapy with observation or bracing depending on their individual circumstances.
Learn more about scoliosis-specific exercises https://scolicare.com/patients-scoliosis-specific-exercise and their role in treatment.
Surgery
When curves exceed approximately 40–50 degrees and continue to progress, surgery may be considered.
The most common surgical procedure is spinal fusion surgery, which aims to:
-
Stabilise the spine
-
Prevent further progression
-
Improve spinal alignment
Surgical decisions are complex and should never be based solely on the Cobb angle.
Factors such as symptoms, age, overall health, function, and quality of life must also be considered.
Important Limitations of the Cobb Angle
Although the Cobb angle is highly valuable, it is not a perfect measurement.
1. Measurement Error Exists
The Cobb angle has an accepted margin of error of approximately ±5 degrees.
Small differences between X-rays may occur because of:
-
Different radiologists
-
Slight changes in patient positioning
-
Time of day
-
Variations in muscle tension and posture
For example, a curve measured at 25 degrees on one X-ray and 28 degrees on another may not necessarily represent true progression.
Clinicians often look for trends over multiple assessments rather than focusing on a single measurement.
2. Scoliosis Is a Three-Dimensional Condition
The Cobb angle only measures the side-to-side curvature of the spine in the coronal plane.
However, scoliosis is actually a three-dimensional deformity involving:
-
Sideways curvature
-
Vertebral rotation
-
Changes in the spine's natural front-to-back curves
This means that two people with identical Cobb angles may look very different clinically.
Some patients with a 25-degree curve may show significant rib prominence, while others may appear relatively symmetrical.
Why the Cobb Angle Is Not Everything in Adult Scoliosis
For adults, the Cobb angle becomes just one component of a much larger clinical picture.
Many adults seek treatment because of symptoms rather than concerns about the curve measurement itself.
Research has shown that the severity of symptoms does not always correlate directly with the Cobb angle.
An adult with a 20-degree curve may experience significant pain, while another individual with a 50-degree curve may remain relatively symptom-free.
Factors Often More Important Than the Cobb Angle in Adults
Pain and Quality of Life
Pain is one of the most common reasons adults seek scoliosis treatment.
Important considerations include:
-
Chronic back pain
-
Fatigue
-
Sleep quality
-
Mental wellbeing
-
Ability to work and exercise
The impact on daily life is often more relevant than the curve measurement itself.
Sagittal Balance
Research demonstrates that sagittal alignment has a major influence on quality of life.
A forward-leaning posture often causes:
-
Increased muscular fatigue
-
Reduced walking endurance
-
Greater pain levels
-
Increased fall risk
In many adult scoliosis cases, restoring postural balance becomes a primary treatment objective.
Neurological Symptoms
Degenerative changes may lead to nerve compression.
Symptoms can include:
-
Leg pain
-
Sciatica
-
Numbness
-
Tingling
-
Weakness
These symptoms often require immediate attention regardless of the Cobb angle measurement.
Risk of Progression
While progression generally slows after skeletal maturity, adults remain at risk.
Studies suggest that adults entering maturity with curves greater than 30 degrees may experience continued progression throughout life.
Degenerative scoliosis may progress by approximately 3 degrees per year in some individuals.
Functional Capacity
The ability to perform daily activities is often more important than the measured curve.
Clinicians assess:
-
Walking tolerance
-
Stair climbing
-
Balance
-
Endurance
-
Fall risk
Treatment should ultimately improve function rather than simply target a specific X-ray number.
The Relationship Between Growth, Hormones, and Cobb Angle Progression
For adolescents, growth and hormonal changes play a major role in curve progression.
Periods of rapid growth can significantly increase the likelihood of curve worsening.
Research has also explored the relationship between hormones, skeletal maturity, and scoliosis progression.
Parents concerned about this topic can learn more in our article discussing hormones and scoliosis progression.
Can the Cobb Angle Improve?
Many patients ask whether their Cobb angle can decrease.
The answer depends on several factors including:
-
Age
-
Skeletal maturity
-
Curve flexibility
-
Treatment approach
-
Consistency with exercise and bracing
Some patients achieve measurable improvements, while others focus on preventing progression and maintaining function.
More importantly, successful treatment should not be judged solely by X-ray changes.
Improved posture, reduced pain, better balance, greater confidence, and enhanced quality of life are equally meaningful outcomes.
Final Thoughts
The Cobb angle remains the gold standard for diagnosing and monitoring scoliosis. It provides clinicians with a reliable and standardised method for assessing spinal curvature and guiding treatment decisions.
However, scoliosis is far more complex than a single number.
For growing children, the Cobb angle helps identify progression risk and determine whether observation, bracing, or scoliosis-specific exercises may be appropriate.
For adults, pain, posture, balance, neurological symptoms, function, and overall quality of life often become even more important than the curve measurement itself.
The most effective scoliosis management combines radiographic findings with a comprehensive assessment of the individual. Understanding the Cobb angle is valuable, but understanding how scoliosis affects the whole person is what truly guides successful treatment.
References:
Schwab, F. J., Blondel, B., Bess, S., Hostin, R., Shaffrey, C. I., Smith, J. S., Boachie-Adjei, O., Burton, D. C., Akbarnia, B. A., Mundis, G. M., Ames, C. P., Kebaish, K., Hart, R. A., Farcy, J. P., & Lafage, V. (2013). Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine (Phila Pa 1976), 38(13), E803-812. https://doi.org/10.1097/BRS.0b013e318292b7b9
Aebi, M. (2005). The adult scoliosis. Eur Spine J, 14(10), 925-948. https://doi.org/10.1007/s00586-005-1053-9
Glassman, S. D., Bridwell, K., Dimar, J. R., Horton, W., Berven, S., & Schwab, F. (2005). The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976), 30(18), 2024-2029. https://doi.org/10.1097/01.brs.0000179086.30449.96
Smith, J. S., Fu, K. M., Urban, P., & Shaffrey, C. I. (2008). Neurological symptoms and deficits in adults with scoliosis who present to a surgical clinic: incidence and association with the choice of operative versus nonoperative management. J Neurosurg Spine, 9(4), 326-331. https://doi.org/10.3171/spi.2008.9.10.326
Ascani, E., Bartolozzi, P., Logroscino, C. A., Marchetti, P. G., Ponte, A., Savini, R., Travaglini, F., Binazzi, R., & Di Silvestre, M. (1986). Natural history of untreated idiopathic scoliosis after skeletal maturity. Spine (Phila Pa 1976), 11(8), 784-789. https://doi.org/10.1097/00007632-198610000-00007
Palazzo, C., Montigny, J. P., Barbot, F., Bussel, B., Vaugier, I., Fort, D., Courtois, I., & Marty-Poumarat, C. (2017). Effects of Bracing in Adult With Scoliosis: A Retrospective Study. Arch Phys Med Rehabil, 98(1), 187-190. https://doi.org/10.1016/j.apmr.2016.05.019