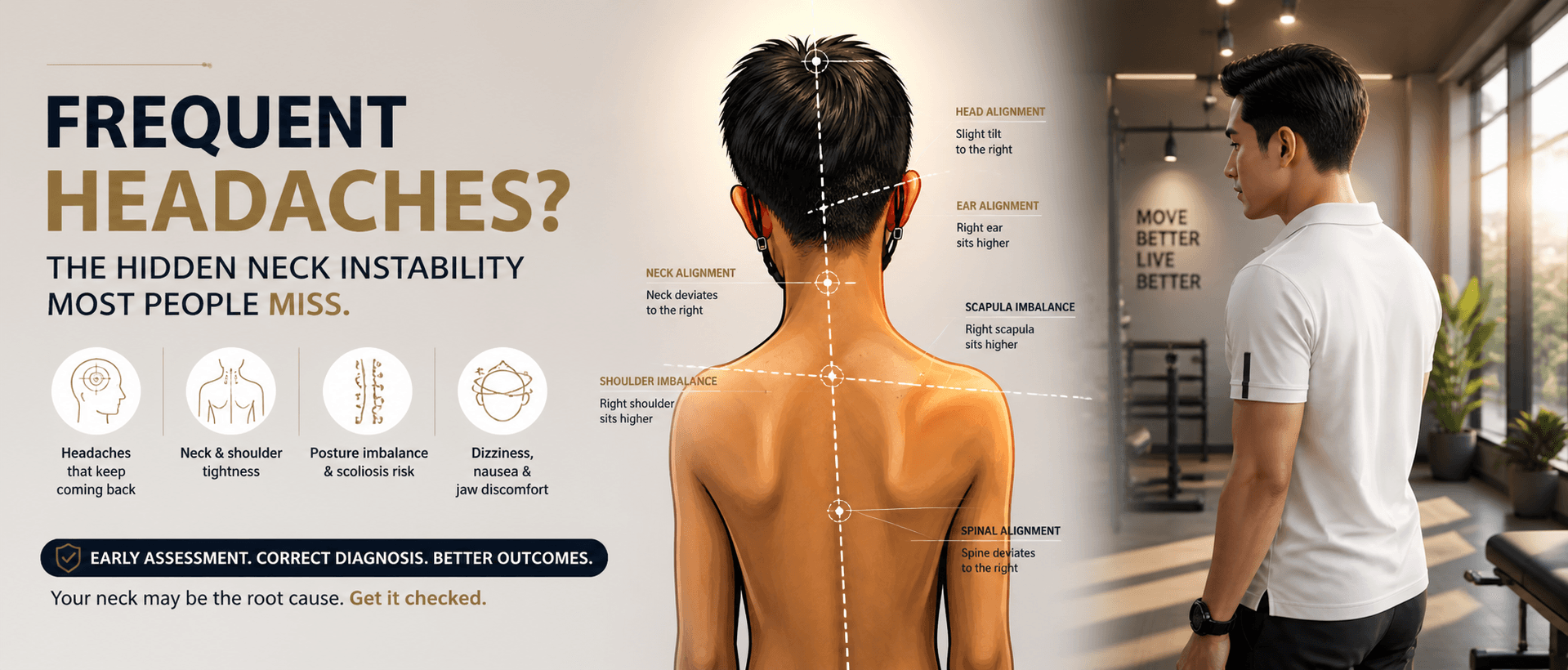
Frequent Headaches? The Research-Backed Reason You Should Check Your Upper Neck (C1–C2)
Most people live with headaches far longer than they should.
They try to manage it—massage, stretching, medication—but the relief is temporary. The headache comes back. The neck tightens again. The cycle continues.
What many patients don’t realise is this:
👉 Persistent headaches are often not just muscular—they can be a sign of instability in the upper neck (C1–C2)
And this is not just clinical opinion.
It is supported by research.
A Real Case From Clinic
A 44-year-old female presented with:
-
Frequent headaches
-
Persistent neck tightness
-
A heavy, pulling sensation at the base of her skull
She had already tried multiple treatments, but nothing held.
On examination, her upper cervical spine did not move normally. A stability screening suggested possible ligament laxity, particularly around C1–C2.
She was referred for imaging.
The findings confirmed:
-
Abnormal cervical rotation
-
Signs of upper cervical instability
Once care shifted toward restoring stability—not just relieving tension—her symptoms began to improve.
This pattern is more common than most people think.
What Research Says: It’s Not Just Muscles
A key paper titled “Chronic Neck Pain: Making the Connection Between Capsular Ligament Laxity and Cervical Instability” highlights a critical concept:
👉 Chronic neck pain and headaches are often driven by ligament laxity, not just muscle tightness
Key research insights:
-
Ligaments—not muscles—are the primary stabilisers of the spine
-
When ligaments become lax or overstretched, joints lose control
-
This leads to excessive motion (instability) and ongoing irritation
-
The result is chronic, recurring symptoms—not one-time pain
In simple terms:
👉 Muscles react
👉 Ligaments control
When control is lost, muscles cannot fully compensate.
Why the C1–C2 Region Is So Important
The C1 (atlas) and C2 (axis) are unique:
-
They account for ~50% of your neck rotation
-
They sit directly below the brainstem
-
They rely heavily on ligament stability
This region is designed for mobility—but depends on precise control.
When that control is compromised:
-
Movement becomes excessive or delayed
-
The nervous system becomes irritated
-
Symptoms begin to appear
The Role of the Alar Ligaments (Research Explained Simply)
The alar ligaments are key stabilisers connecting the skull to C2.
Research shows they:
-
Limit rotation and side bending
-
Maintain head–neck alignment
-
Protect the brainstem and spinal cord
What happens when they become lax?
Biomechanical studies demonstrate:
-
Increased rotation and side bending at C1–C2
-
Loss of precise movement control
-
Development of instability
👉 This is not theoretical—this is measurable in controlled studies
How Instability Creates Your Symptoms
The research highlights an important mechanism:
👉 Instability causes repetitive microtrauma, not just one injury
Over time, this leads to:
-
Chronic headaches
-
Neck stiffness and muscle guarding
-
Dizziness and nausea
-
Jaw discomfort
-
Reduced coordination and balance
Because the upper cervical spine is rich in mechanoreceptors (position sensors), instability also disrupts how your brain perceives movement.
👉 This is why symptoms feel inconsistent—but persistent
Why Screening (Like the Alar Ligament Test) Is Encouraged
Clinical research supports the use of upper cervical stability tests as part of proper assessment.
The Alar Ligament Test is one such screening tool.
Research-supported reasons to test:
-
Patients with headaches, neck pain, dizziness should be screened
-
The test helps identify abnormal motion and loss of control
-
It has moderate to high specificity, meaning positive findings are meaningful
-
It is recommended as a safety step before cervical treatment
👉 This is key:
The purpose of testing is not to diagnose everything—
It is to avoid missing instability
Why This Matters Before Treatment
Research strongly emphasises:
-
Treating the neck without screening stability can be inappropriate
-
Instability changes how the spine should be managed
-
Proper assessment reduces risk and improves outcomes
👉 Good care is not about doing more
👉 It’s about knowing what you are dealing with
The Bigger Picture: From Neck Instability to Posture & Scoliosis
Your body prioritises one thing:
👉 Keeping your eyes level
If the top of your neck (C1–C2) is unstable:
-
Your head may tilt subtly
-
Your shoulders compensate
-
Your spine adapts
Over time, this may contribute to:
-
Postural asymmetry
-
Uneven shoulder height
-
Early scoliosis patterns
Research has shown that scoliosis patients often present with:
-
Upper cervical asymmetry
-
Altered head positioning
-
Imbalance at the craniovertebral junction
👉 The spine doesn’t just curve randomly
👉 It adapts to what happens above it
What You Can Do Today
If you experience:
-
Frequent headaches
-
Neck tightness
-
Dizziness or jaw discomfort
-
Symptoms that keep returning
Start simple:
-
Observe your posture from behind
-
Look for asymmetry in your head and shoulders
-
Notice patterns—not just pain
Then take the next step:
👉 Get properly assessed
Final Takeaway (Research-Based)
-
The C1–C2 region controls half of your neck rotation
-
The alar ligaments are key stabilisers of this system
-
Research shows ligament laxity leads to instability and chronic symptoms
-
Patients with headaches and neck symptoms should be screened—not assumed
-
The Alar Ligament Test is part of safe, evidence-based assessment
Most importantly:
👉 Persistent headaches are not random
👉 They are often a sign of lost stability, not just tight muscles
And in many cases, the answer begins here—
At the top of your spine, where control matters most.